
Juerg Martin Burren, reviewed by Professor Andreas Schibler
Modes of ventilation can at first seem like a maze. However as long as you understand the basics you will be able to operate any ventilator. In this article, we want to provide a way to understand the basic aspects of different ventilation modes that are commonly used.
Mini-physics
As a general principle, intensive care ventilators use gas flow generated by either a turbine or valves controlling fresh gas flows (O2, Air). This flow generates pressure and therefore changes lung volume depending on the respiratory system’s compliance.
There is one crucial physics aspect that we need to talk about before getting started – Compliance.
Compliance describes the amount of volume generated by a certain pressure


The total compliance of the respiratory system is the sum of the lung’s and chest wall’s compliance.


Normal compliance in paediatric patients is ~1ml/cmH2O/kg Ideal Body Weight (IBW) up to 25kg of IBW. With increasing weight the compliance per kg IBW decreases continuously down to adult values of approximately 0.4-0.6ml/cmH2O/kg IBW.
Theoretical aspects of ventilation modes
Volume controlled (VC) ventilation is where both volume and flow are controlled. Normally, flow is set to a fixed amount, meaning volume increases linearly over time up to the tidal volume (TV) chosen by the operator. Because flow, TV and compliance are given – the pressure needed to generate the TV is the dependent on the compliance. This is consistent with the following formula:

- The higher the TV with a static compliance the higher the pressure needed to achieve it and vice versa
- The higher the compliance the lower the pressure needed to generate a given TV and vice versa
- This means that the ventilator will adapt the pressure it applies as the compliance changes over time
Flow and pressure during volume controlled ventilation

- Set TV and Ti
- Ventilator applies constant flow until TV reached
- PIP and Pplat depend on the compliance and resistance of the respiratory system
- Maintains quasi-static minute volume and therefore quasi-constant CO2 level
- Lower Mean Airway Pressure (MAP) than pressure controlled ventilation resulting in slightly less oxygenation and a higher risk of de-recruitment
Pressure controlled (PC) ventilation is where pressure and flow are controlled by the ventilator/operator. Peak Inspiratory Pressure (PIP) is set for a specific duration (inspiratory time, Ti). Because pressure, time and compliance are given, the TV generated is dependent on the compliance of the respiratory system. This is consistent with the following formula:

- The higher the pressure or compliance, the higher the TV and vice versa
- The TV and therefore minute ventilation (and CO2 control) will change as the compliance changes over time
Flow and pressure during pressure controlled ventilation

- Set PIP and Ti
- Ventilator applies decelerating flow pattern to reach PIP fast and then maintain it
- TV and therefore minute ventilation depends on respiratory system compliance and resistance
- Varying minute ventilation and therefore CO2 level
- Higher MAP compared to volume controlled modes resulting in better oxygenation
- Potentially more comfortable for patients
What is a breath?
- A breath is a cycle of positive flow (inspiration) and negative flow (expiration)
- Inspiratory time (Ti) is defined as the period from the start of positive flow to the start of negative flow
- Expiratory time (Te) is defined as the period from the start of expiratory flow to the start of inspiratory flow.
- Expiration is longer than inspiration during positive pressure ventilation because the process is passive and the driving force is reduced across the duration of exhalation
- The usual ratio for inspiration to expiration is 1:2
Assisted vs unassisted breaths
- An unassisted breath is one for which the ventilator simply provides the inspiratory flow demanded by the patient
- An assisted breath is one during which the ventilator provides additional support in form of pressure or volume (Pressure / Volume Support)
Classification of breaths
Below is an adapted version of the Chatburn classification. First, the patient, or the machine, can either trigger (start) or cycle (stop) inspiration.
| Trigger | Cycle |
| Patient triggering means starting inspiration based on a patient signal independent of a machine trigger signal. | Patient cycling means ending inspiratory time based on signals representing the patient’s efforts. Flow cycling is a form of patient cycling used in pressure support ventilation |
| Machine triggering means starting inspiration based on a signal from the ventilator, independent of a patient trigger signal | Machine cycling means ending inspiratory time independent of signals from the patient |
Second, breaths can be spontaneous or mandatory.
A spontaneous breath is a breath for which the patient retains control over timing.
This means that the start and end of inspiration are determined by the patient, independent of any ventilator settings for inspiratory and expiratory times. That is, the patient both triggers and cycles the breath.
A mandatory breath is a breath for which the machine triggers and/or cycles the breath.
The patient has lost control over timing of the breath. A mandatory breath is, by definition, assisted. This results in 3 breath sequences:
- Continuous Mandatory Ventilation (CMV) – spontaneous breaths are not allowed. All breaths are mandatory because every patient-triggered signal in the trigger window produces a ventilator-cycled inspiration (ie, a mandatory breath).
- Intermittent Mandatory Ventilation (IMV) – spontaneous breaths may occur between mandatory breaths
- Continuous Spontaneous Ventilation (CSV) – all breaths are spontaneous
Don’t be confused about CMV – It includes modes in which every breath shape and duration is controlled by the machine which therefore makes it a mandatory breath. The “mandatory” bit therefore relates to how the breath looks like. In other words, CMV does not allow for any other breaths than the set ones. This means that there is no pressure support or volume support because these breaths would look differently. Every time the patient triggers, a full “mandatory breath” is delivered.
Ventilatory patterns
Using the classification above gives us 5 basic ventilatory patterns.
| Ventilatory pattern | Other names |
| Volume Control – CMV | Assist/Control, A/C, CMV, Volume Assist / Control, Volume Control |
| Volume Control – IMV | Synchronized Intermittent Mandatory Ventilation, SIMV |
| Pressure Control – CMV | Assist/Control, A/C, CMV, Pressure Assist / Control, Pressure Control |
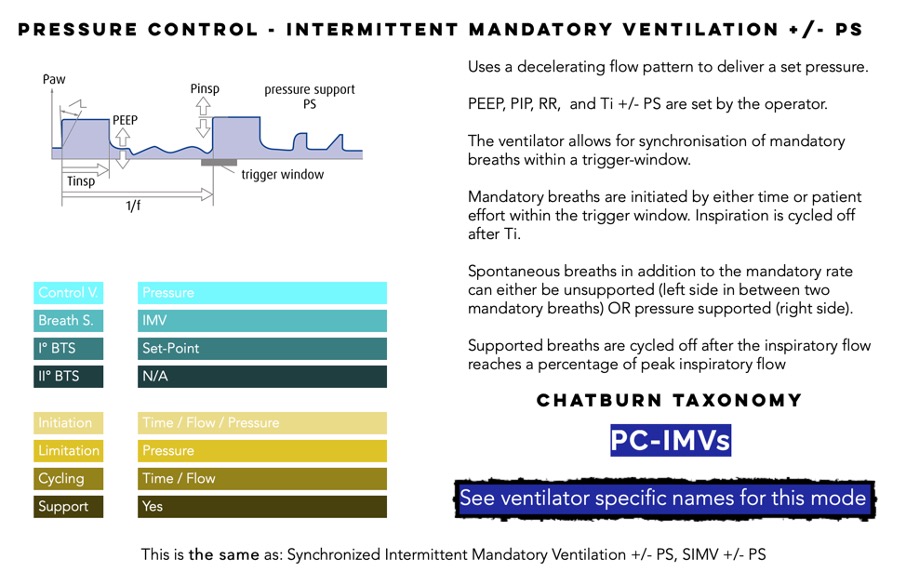
| Pressure Control – IMV | Synchronized Intermittent Mandatory Ventilation, SIMV |
| Pressure Control – CSV | Spont, Spontaneous |
Targeting scheme
Within each ventilatory pattern there are several variations that can be distinguished by their targeting scheme(s). A targeting scheme is a description of how the ventilator achieves preset targets. The targeting scheme is what distinguishes one ventilatory pattern from another. There are a number of basic targeting schemes that comprise the wide variety seen in different modes of ventilation:
- Set-point: The operator sets all the parameters of the pressure waveform (pressure control modes) or volume and flow waveforms (volume control modes)
- Dual: Allows the ventilator to switch between volume control and pressure control during a single inspiration
- Bio-variable: Allows the ventilator to automatically set the inspiratory pressure or tidal volume randomly to mimic the variability observed during normal breathing
- Servo: Inspiratory pressure is proportional to inspiratory effort
- Adaptive: Allows the ventilator to automatically set one target (eg, pressure within a breath) to achieve another target (eg, average tidal volume over several breaths)
- Optimal: Automatically adjusts the targets of the ventilatory pattern to either minimize or maximize some overall performance characteristic (eg, minimize the work rate done by the ventilatory pattern)
- Intelligent: Uses artificial intelligence programs such as fuzzy logic, rule based expert systems, and artificial neural networks
The targeting schemes can be represented by single, lower case letters: set-point = s, dual = d, servo = r, bio-variable = b, adaptive = a, optimal = o, intelligent = i.
A targeting scheme is a description of how the ventilator achieves preset targets.
Mode of ventilation
Using everything that’s been covered, we finally arrive at the mode of ventilation. A mode of ventilation is classified according to its control variable, breath sequence, and targeting scheme(s). The taxonomy is based has 4 hierarchical levels:
- Control Variable (Pressure or Volume for the primary breath)
- Breath Sequence (CMV, IMV, or CSV)
- Primary Breath Targeting Scheme (for CMV or CSV)
- Secondary Breath Targeting Scheme (only for IMV)

So how do all these modes apply to the ventilator in front of you when you’re next in an intensive care unit? Below are some of the common ventilation modes that you will come across, and how each of them can be broken down and translated into the individual components that we have mentioned already.






Juerg Martin Burren is also the owner and creator of PIVARES. PaediatricFOAM enjoyed collaborating with the PIVARES team on this article and is grateful to PIVARES for allowing their images to be used in this article. To find out more about PIVARES, feel free to visit their website at https://www.pivares.com