
Dr Khadiga Hussien, Paediatric ST5 trainee; Dr John Madar (Consultant Neonatologist) Plymouth University Hospital, UK
Whether you’re new to NICU or stepping up to take more responsibility as a registrar, those little blood gas print-outs follow you round like a paper trail. The more comfortable you feel interpreting them, the less anxiety your NICU shifts will hold!
Blood gas measurement is the gold standard for evaluating ventilated babies in the NICU, as it gives you a clear picture of the baby’s acid-base balance and oxygenation. In the NICU, blood gases are used to guide ventilation strategies in critically ill newborns, including extremely preterm babies.
BUT! The interpretation of blood gases in neonates – especially in extreme prems – can be quite challenging, as their physiology and metabolism may be different to that of older children and adults. Also, certain ‘abnormal’ blood gas findings can have greater or lesser significance depending on the gestational age and clinical context of the baby.
In this article, we’re going to give a practical and detailed overview of blood gas interpretation in NICU babies. We’ll go through different blood gas parameters, including ‘normal’ and ‘acceptable’ ranges, how to interpret the results in a clinical setting, and the importance of sample type and technical errors.
We’ll also give you some practical tips and clinical correlations to help you understand the significance of blood gas values in the management of neonates. By the end of this review, we hope you have a good understanding of how to interpret and use blood gas results to guide ventilation strategies.
Please keep in mind that although blood gas analysis is super important, it’s only one part of a full assessment of a baby’s acid-base balance and oxygenation status. Other things, (such as clinical presentation, haemodynamics, and imaging) also need to be considered when making any ventilation decisions.
Blood Gas Parameters

On modern blood gas machines, you can adjust the temperature and oxygen consumption parameters to give you more accurate readings. As well as blood gases, most machines in UK NICUs also measure electrolytes, haemoglobin, and bilirubin.
Here’s a quick overview of some of the main blood gas parameters, with some of their clinical implications.
pH
Normal value (7.35 – 7.45)
pH is a measure of the concentration of extracellular hydrogen ions, represented by the negative logarithm of the hydronium ion (H3O+). More hydrogen ions = low pH; fewer hydrogen ions = high pH. The body carefully regulates pH within a range that cells can function in. There are many buffer systems that keep the pH within range; the carbonic acid-bicarbonate buffer system is the most important of these.
CO2 + H2O <-> H2CO3 <-> H+ + HCO3 –
Henderson-Hasselbalch equation
The lungs and kidneys also help with pH regulation by getting rid of volatile and fixed acids, respectively, and by controlling bicarbonate concentrations.
While buffer mechanisms can help get pH back towards normal levels, they may not result in full correction. It’s essential to maintain the appropriate pH to make sure cells can function properly.
NICE Guidelines recommend accepting permissive hypercapnia in preterm neonates on invasive ventilation and taking action if hypocapnia is detected.
PaCO2
Normal Value (4.6 – 6.0 kPa)
PaCO2 (partial pressure of arterial carbon dioxide) is a measure how much CO2 is dissolved in the blood. CO2 is 20x more soluble in the blood than oxygen and it’s mainly transported by bicarbonate. In the lungs, CO2 is converted back into gas and exhaled. In blood gas interpretation, PaCO2 can tell us about the efficiency of gas exchange. Insufficient ventilation or impaired gas exchange can cause abnormal PaCO2 levels.
PaO2
Normal Value (7.0 – 12.0 kPa in Term, 6.5 – 10.5 kPa in Preterm)
PaO2 represents oxygen dissolved within the plasma, and is a good measure of a baby’s oxygenation status. Only arterial blood gives an accurate measure of PaO2. . PaO2 only measures free oxygen and doesn’t account for oxygen bound to haemoglobin, which is known as oxygen saturation. Oxygen saturation can be measured directly in arterial blood (SaO2) or estimated by pulse oximetry (SpO2).
The relationship in blood between oxygen saturation (SO2) and partial pressure (PO2) is represented by the oxygen–haemoglobin dissociation curve. Abnormal PaO2 levels indicate respiratory or circulatory problems.
Bicarbonate (HCO3 ¯)
Normal value (22-26 mEq/L in Term, 20- 24 mEq/L in Preterm)
Bicarbonate isn’t directly measured by the blood gas machine, – it is calculated from the measured values of pH, PaCO2, and total CO2. A decrease in bicarbonate concentration in the blood can indicate metabolic acidosis. This happens when bicarbonate is used up neutralizing acids.
Base excess (BE)
Normal Value (-2 to +2)
The blood gas machine calculates ‘base excess’ based on the values of pH and bicarbonate. Base excess indicates the amount of acid or base that would be needed to return the pH to a normal level of 7.4 in the presence of normal levels of carbon dioxide (PaCO2).
Lactate
Normal value (< 2.0 mmol/ L)
The lactate level reflects the body’s metabolic status. Elevated lactate levels may indicate that there is not enough oxygen and the body is relying on anaerobic metabolism to produce energy. High lactate can suggest a serious underlying condition, such as sepsis, tissue hypoxia or shock; a baby with a high lactate needs urgent clinical assessment.
Anion gap
The anion gap (AG) is a measure of the difference between the cations (+) and anions (-) in the plasma. It is calculated with this equation:
AG = (Na+) – (Cl– + HCO3–)
The normal range of AG is between 10 and 14 mmol/l (if potassium is included in the calculation, the normal range is 14 to 18 mmol/l). Most of the normal AG is due to the negative charges of plasma proteins, particularly albumin. So, when acute illness or injury lower the plasma albumin, the AG falls.
Losing bicarbonate from the gut or kidney can cause normal anion gap acidosis, characterized by low serum HCO3– levels but a normal anion gap. This can happen in neonates, particularly premature babies, due to their immature kidneys’ low bicarbonate threshold and their reduced ability to secrete acids and ammonium.
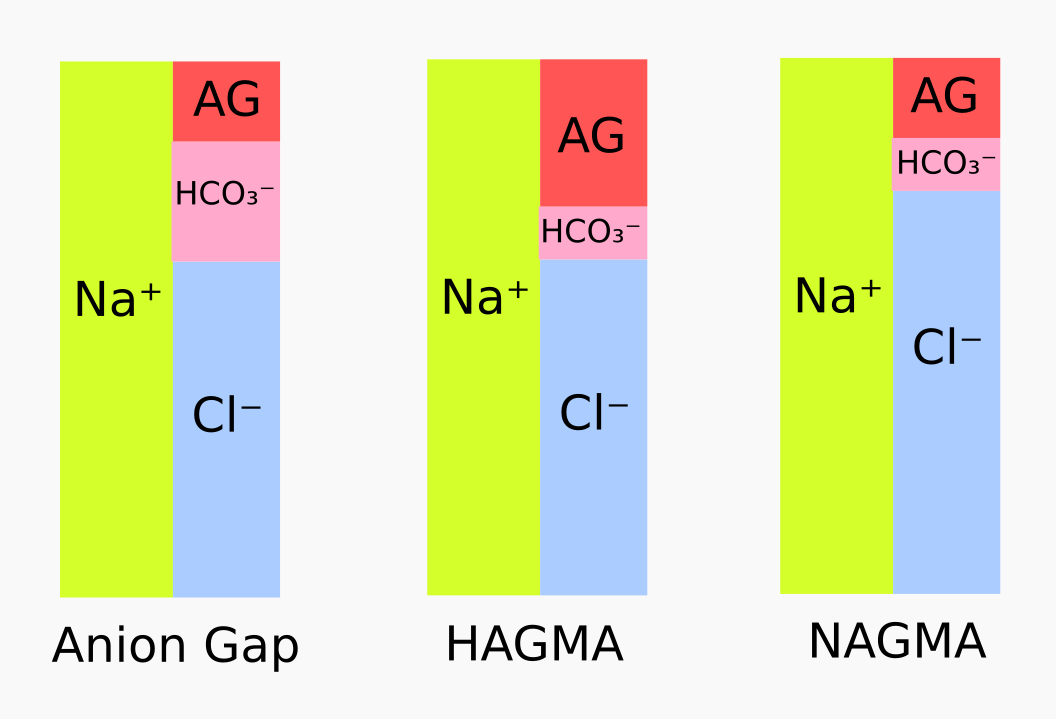
Lactic acidosis can cause high anion gap acidosis in neonates when there is hypoxemia caused by things like perinatal asphyxia, severe lung disease, sepsis, or myocardial dysfunction, amongst others. Severe acidosis caused by metabolic disorders is rare, but should always be considered as a possibility.
Understanding the Different Types of Blood Gas Samples in Ventilated Babies
The three types of blood gas sample that you can use to monitor a ventilated baby: arterial, venous, and capillary. You must always know which type of sample has been taken – this will influence which parameters you need to take into account when interpreting results.

Arterial blood samples are the ‘best’ (most accurate) for monitoring ventilated babies and are usually taken from an arterial line (umbilical or peripheral). Pragmatically, not all babies have arterial lines, so sometimes a compromise is necessary.
Venous blood is the least useful sample for monitoring a ventilated baby, as it can’t be used to work out the oxygenation index (OI) or partial pressure of oxygen (PO2). Compared to arterial samples, central venous (from umbilical venous line) pH is usually 0.03 to 0.05 units lower, PCO2 is usually (0.5-0.7 kPa) higher, and bicarbonate (HCO3) doesn’t increase significantly. Peripheral venous pH is approximately 0.03 to 0.04 units lower than arterial pH, HCO3 is about 2-3 mEq/L higher, and PCO2 is about (0.4-1 kPa) higher.

Capillary blood gases may be easy to take, but samples are easily affected by cold extremities, poor perfusion, and squeezing, which can all give inaccurate results. A free-flowing capillary gas can give a decent estimate of PCO2.
Interpreting and acting on blood gas results in eight steps
Note that lower values are used for extreme preterms
- Is the pH acidotic or alkalotic?
- If pH < 7.35, the patient has acidosis
- If pH > 7.45, the patient has alkalosis
- If pH is acidotic, what’s the main source of acid?
- If PCO2 > 6kPa, the acidosis is respiratory
- If HCO3 – < 20 mEq/L, the acidosis is metabolic
- If PCO2 > 66kPa and HCO3 – < 20 mEq/L, the acidosis is mixed
- If pH is alkalotic, what’s the main source of base?
- If HCO3 – > 24, the alkalosis is metabolic
- If PCO2 < 4, the alkalosis is respiratory
- If HCO3 – > 24 and PCO2 < 4, the alkalosis is mixed
- Is the pH derangement is compensated, partially compensated, or uncompensated:
- If the pH is normal despite an acid-base imbalance, this means that the body has fully compensated for the imbalance. E.g. if the pH is normal and the level of carbon dioxide (CO2) and bicarbonate (HCO3–) is high, respiratory acidosis has been fully compensated for by metabolic alkalosis.
- If the pH is outside the normal range, but the body has partially compensated for the acid-base imbalance, the pH derangement is considered partially compensated. If, for example, the pH is low (acidotic) and the CO2 level is high and the HCO3– level is high, but the pH hasn’t returned to a normal level, respiratory acidosis is considered partially compensated by metabolic alkalosis.
- If the pH is outside the normal range and there is no compensatory response by the body, the pH derangement is uncompensated. For example, if the pH is low (acidotic) and the CO2 level is high but the HCO3– level remains normal, respiratory acidosis is considered uncompensated.
- Check oxygenation (PaO2) if it’s an arterial sample. If PaO2 is low, this could indicate hypoxemia.
- What’s the lactate? Interpret it along with other parameters.
- Think about whether the baby’s ventilation settings need adjustment – based on clinical stability, previous changes made, and accessibility
- When does the next blood gas need to be done?
- For stable patients, blood gases can be checked every 6-8 hours
- For critically ill babies, blood gases need to be checked more frequently (sometimes as regularly as every 30 minutes to an hour) if there are major changes in the patient’s condition.
Are you still with us?! A little check of understanding 🙂
How do you interpret these blood gas values:
pH 7.32, pCO2 9.61 kPa, pO2 8.24 kPa, HCO3– 31.6 mmol/L, BE 11.1, Lac 0.87
Don’t cheat! Answer below 🙂
.
.
.
.
.
.
.
.
Answer:
- The pH of 7.32 is lower than the normal range, indicating acidosis.
- The pCo2 level of 9.61 kPa is elevated, indicating respiratory acidosis as the source of acidosis.
- The HCO3– level of 31.6 mmol/L is above the normal range, indicating that the body is trying to compensate for the acidosis.
- However, the pH is still not fully back to the normal range, indicating that the compensation is partial.
- The pO2 level of 8.24 kPa is within the normal range.
- The lactate level of 0.87 is also within the normal range, along with pO2 indicating normal oxygenation and adequate tissue perfusion.
What can cause errors in blood gas results?
Just like with all laboratory tests, if there are technical errors, you get dodgy results. If you are in doubt, repeat it before attempting to act on it! Here are some of the common causes of errors and how to prevent them:
Air bubble

Bubbles in the sample will lower the PaCO2, as the analyzer can’t accurately measure the amount of CO2 in the sample. An air bubble can also raise or lower
the PaO2, depending on how big the bubbles are. So it’s really important to make sure your sample is bubble free – be gentle when handling the sample and allow it to settle before putting it into the machine.
Delays
It’s so easy to get sidetracked on a busy NICU! But that sample needs to get processed ASAP – leave it too long and

the red blood cells carry on consuming oxygen and producing carbon dioxide in the blood gas tube, making the measurements inaccurate.
If there’s no chance of processing a sample straight away, it’s possible to slow down metabolism and preserve the sample by putting it in ice water. Studies have shown that when a blood gas sample is stored in ice water, the PaO2 and SaO2 remain stable for up to 30 minutes. PaCO2, however, increases significantly after 20 minutes, and lactate levels increase after 15 minutes.
In conclusion –
Contamination with intravenous fluids
IV fluids can dilute the sample and change the concentrations of various components being measured (e.g. electrolytes). A sample diluted with IV fluid might not be affected in pH, but the PaCo2 will typically be lower which would increase the base deficit.
Following the proper procedure for taking samples (especially from an arterial line) will make sure your sample is not diluted with any fluids.
Temperature correction
Temperature influences measurements of blood gases such as pH, partial pressure of carbon dioxide (pCO2), and partial pressure of oxygen (pO2). When blood is at a higher temperature, the pH and pCO2 values will be higher, the pO2 values will be lower and vice versa.
Modern blood gas machines use electrodes that compensate for body temperature or include built-in temperature sensors that can adjust the results according to either a standard body temperature or one that is manually entered. Without this correction, the results can be off by as much as 0.05-0.1 pH units or 1.3-2.6 kPa for pCO2 and pO2.
Conclusion
Being able to properly interpret blood gases is crucial in caring for NICU babies – understanding the various types of blood gas sample and the normal values for each parameter while having a solid step-by-step approach to interpretation (and to be aware when misleading values may have been caused by sampling errors).
It’s important to always take a baby’s clinical context into account – including their ventilation status and other parameters – remember that in extreme preterms, lower values can sometimes be allowed when you are aiming for a ‘gentle’ approach to ventilation.
Following the tips we have given, plus the guidelines set by your unit, will help you make sure that you always provide the best care for your smallest patients.
Authors: Dr Khadiga Hussien and Dr John Madar
References
Brodsky, D., & Martin, C. (2003). Neonatology review
Chakravarty, S. (2008). Neonatal ventilation made easy
DynaMed. (n.d.). Acid-base abnormalities – Approach to the patient
Gillham, M., & Sidebotham, D. (2007). Acid-Base Disturbances In Cardiothoracic critical care
Petty, J. (2013). Understanding neonatal ventilation: Strategies for decision making in the NICU
Very good article, well done